
Above photo: Masks were important during the 1918 influenza pandemic, with no vaccine and no antibiotics for pneumonia.
In all epidemics, there are some principles which determine how well communities and nations will respond, how long the crisis will last and how soon there will be recovery. We can already draw some lessons from the very big differences between particular countries in the COVID-19 pandemic, in particular why some wealthy nations like the UK and the USA are amongst the hardest hit. Although the numbers infected are still rising and the impact has not yet peaked, in most countries, we are entitled to ask: why have some countries controlled infections and minimized deaths better than others? This question, I suggest, leads us to consider principles of public health systems, of health planning and of broader social coherence. In particular, we should observe renewed evidence which affirms that public health systems are best able to develop the planning, prevention measures and coordination necessary to deal with epidemics.
The year 2020 saw the rise of a global epidemic (a pandemic) with a new variety of coronavirus which attacks human respiratory systems. This virus is highly infectious, if not highly fatal, compared to the recent epidemics of SARS-1 and MERS. COVID-19 seems deadly mainly to the elderly and the unwell (Doherty 2020). Extremely restrictive measures have been applied across much of the globe, while health systems try to contain the crisis and work out how best to prevent and treat it.
Nevertheless, extraordinary levels of skepticism about the state in western societies have aggravated reactions to severe quarantine measures, leading some to question whether the epidemic even merits emergency attention. This is while we see reports of more than a thousand deaths every day in the USA, China’s recovery after its extreme ‘lockdown’ measures, the scandal of dead bodies on the streets of Guayaquil in Ecuador (Gallón 2020), and while Cuban doctors help deal with the crisis in many countries (AP 2020). Skepticism has become cynicism in many western countries, due to a deep distrust of governments and their corporate partners. Undoubtedly powerful opportunists will exploit this crisis. Large corporations will automate and shed labor, some local authorities will extend arbitrary powers and Washington will persist with its economic and ‘regime change’ wars, using COVID-19 rationales where possible.
But this is a real public health crisis and it would be a mistake to ignore the fact that public health is, in itself, a central battleground. The same financial oligarchies that drive war and corporate privilege also block or colonize public health systems, which they see as multi-billion dollar milk cows. If individual liberties remain the central focus of critique, without recognition of the role of health systems, neoliberal ideologies will simply respond, as usual, on the ‘individual right’ to choose health insurance and to avoid ‘authoritarian’ public health systems. In the current crisis the principal alternatives we see to rapid response, protective public health measures is a neoliberal state which prevaricates, then resorts to heavy-handed policing and its armed forces for social control (Haynes 2020; Browne 2020), when the crisis is undeniable and there is no adequate health workforce.
This is a comparative study of the COVID19 phenomenon, drawing on established principles of public health and epidemic control and making use of the best available epidemiological evidence. It aims to identify and articulate lessons about health systems. Key examples used are the USA and the UK, contrasted with China and South Korea. The Anglo-American duo have stressed more privatized health systems in recent decades, while both China and South Korea have moved from private insurance-based systems to near-universal coverage systems with national planning bodies and increased public investment in their health systems (Dai 2009, Qingyue, Hongwei, Wen, Qiang and Xiaoyun 2015; Kwon, Lee and Kim 2015). The comparison is not, therefore, between capitalist and ‘socialist’ or non-capitalist systems, but rather between systems which have weakened or reinforced their universal health guarantees and health planning commitments.
After some comments on the origins of COVID-19, and on general principles of epidemic control, I examine the interim evidence of differential impact in several countries. The conclusions are over which systems are best prepared, which will minimize casualties and which will recover sooner. These understandings deserve consideration in their own right.
1. The Origins of COVID-19
Much is still unknown about the origin of the new coronavirus, and many of the early claims seem unfounded. A necessary agnosticism should accompany any honest study of this question of origin. COVID-19 (also called SARS-CoV-2) is the latest in the family of RNA coronaviruses, and at least 58 haplotypes (genetic varieties) have been identified, half from inside China and half from outside (Yu, Tang and Corlett 2020). China sequenced and published the virus genome in mid-January (Cohen 2020a) and since then Italian studies isolated and have been sequencing the genome of the Italian virus, showing a particular strain, slightly distinct from the Chinese varieties (Bergna 2020). Many new flu viruses come from animals, and COVID-19 has a possible link to coronavirus haplotypes found in bats (Yu, Tang and Corlett 2020). The first recorded mass outbreak of infections came from the Huanan Seafood Market in Wuhan city, China.
However, notice the difference between ‘first recorded outbreak’ and ‘the origin’. There are several now which suggest that COVID-19 did not have its origins in Wuhan. This parallels the terrible ‘Spanish Flu’ epidemic of 1918-19, which is now generally thought to have not come from Spain. In that pandemic, where millions died, the flu was traced back to migrant workers from France, making it “unlikely” that the 1918 A(H1N1) influenza virus originated in Spain (Trilla, Trilla and Daer 2008). John M. Barry, in the Journal of Transnational Medicine, reviewed the literature on the origins of the 1918 pandemic and, drawing on US, British and Australian studies, concluded that “the most likely site of origin was Haskell County, Kansas”. This county, an isolated area with many farm animals, had an outbreak of a virulent flu in January 1918, a flu which killed healthy young men. That flu spread to an army camp at Funston, and from there was carried to the war fields in France (Barry 2004). Australian Nobel laureate MacFarlane Burnet wrote that the evidence was “strongly suggestive” that the disease started in the United States and spread with “the arrival of American troops in France” (Burnet and Clark 1942). Barry concludes by saying “the fact that the 1918 pandemic likely began in the United States matters because it tells investigators where to look for a new virus. They must look everywhere” (Barry 2004).
An early Chinese genetic study suspected that COVID-19 came to Wuhan from elsewhere. This analysis suggested that the virus “was potentially imported from elsewhere; the crowded market then boosted SARS-CoV-2 circulation” (Yu, Tang and Corlett 2020). Another Chinese study of the first 41 patients admitted to hospital and diagnosed with COVID-19, observed that 27 (66%) “had been exposed to Huanan seafood market” (Huang et al 2020), but 13 (33%) had not. “That’s a big number, 13 , with no link” said infectious disease specialist Daniel Lucey of Georgetown University (Cohen 2020). Professor Robert Garry, from the University of Tulane in New Orleans, also pointed out “our analyses, and others too, point to an earlier origin than [Wuhan]. There were definitely cases there, but that wasn’t the origin of the virus” (Holland 2020). Then a British study, looking at 160 varieties and combining them in three groups, with A as the ancestral strain, found that most of the COVID19 varieties from Wuhan and from east Asia were Type B and non-ancestral (Forster, Forster, Renfrew and Forster 2020).
The transmission path was not well anticipated. Later genomic studies showed that most cases of the outbreak in New York came from Europe; these cases were detected late, due to a lack of testing. Presidents Trump’s 31 January entry ban on people from China had no impact on this source of infection (Zimmer 2020). Later links were found to US warships and US military bases (Arkin 2020).
Many new viruses come from animals, and COVID-19 may have an ancestral link with coronavirus strains found in bats; however no definite link of this sort has been established with the Wuhan outbreak. Nevertheless, western media showed video of a Chinese woman eating a cooked bat, suggesting a Chinese origin. The BBC has pointed out this was from a 2016 travel show, shot on the Pacific island of Palau (BBC 2020).
Importantly, there are reports of earlier cases in both Italy and the USA. In northern Italy local doctors remember “a very strange pneumonia, very severe, particularly in old people” in November and December of 2019. That may mean that “the virus was circulating [there] … before we were aware of this outbreak occurring in China” (Poggioli 2020). The first cases in the USA have also been linked to the many flu deaths throughout 2019. When Centre for Disease Control (CDC) Director Robert Redfield was asked whether some of the US ‘flu deaths’ might have been COVID19, and wrongly diagnosed, he replied “some cases actually have been diagnosed [that way] in the US to date” (New China TV 2020). This raised the possibility of 2019 cases in the USA, perhaps before Wuhan’s December 2019 outbreak. That admission led Chinese official Lijian Zhao to demand ‘transparency’ from the US: “When did patient zero begin in the US? How many people are infected … be transparent! Make public your data! US owes us an explanation” (Zhao 2020). The CDC’s acknowledgement of early and perhaps widespread infections in the USA was reinforced by estimates from the Director of the Department of Health in the state of Ohio, Amy Acton. She was reported as saying that “the fact of community spread says that at least 1 percent … is carrying this virus in Ohio today … over 100,000” (Sullivan 2020). However the matter of 2019 infections and deaths in Italy and the USA is as yet unresolved.
There have also been suggestions that the virus may have come the biological warfare laboratories of the US military. Suspicions were aroused by the sudden closure of the US army’s bioweapons research centre at Fort Detrick in Maryland, in August 2019. This closure was due to fears that “contaminated waste” or agents such as Ebola, smallpox and anthrax could leak from the facility (Wyatt 2020). There was also the presence of US soldiers at the Military World Games in Wuhan in October 2019, just before the Wuhan outbreak. Both issues create grounds for suspicion, yet no direct link has as yet been established. One group of mostly US-based scientists, looking at the characteristics of the virus, have asserted that SARS CoV-2 was “not a laboratory construct” but had natural origins (Anderson, Rambaut, Lipkin, Holmes and Garry). However the better view of their report – hedged with “likely”, “probably”, “not been described” (i.e. no evidence) and “we do not believe” qualifiers – is that they could find ‘no evidence’ of a laboratory origin. So evidence on this matter also remains unresolved.
Overall, there are several sources of evidence that suggest COVID-19 did not originate in Wuhan, nor its seafood market, although that was the first recorded largescale outbreak. Politicised talk of a ‘Chinese virus’ parallels the misnaming of the 1918 pandemic as ‘Spanish Flu’. Most other claims are not well founded. In these circumstances an agnostic approach, open to new evidence, is necessary if we want to really understand the origin of COVID19.
2. Principles of epidemic control
In 2018 the WHO, writing of ‘challenges and risk factors’ for epidemics, spelt out some contemporary risk factors and emphasised key features of an effective response. Current risk factors are aggravated by greater international travel, growing peri-urban areas which have contact with animals, the massive displacement of people by wars and disasters, the overuse of antibiotics which has created microbial resistance, new hazardous agricultural practices and “poor health care systems that have inadequate infection prevention and control practices” (WHO 2018: 25-26). Effective responses to an epidemic require early detection, then containment measures followed by control and mitigation then, if possible, elimination or eradication (WHO 2018: 28-30)
Health researchers have repeatedly argued that “to accurately predict, plan, and respond to current and future influenza pandemics, we must first better understand the events and experiences of 1918 … we must remain vigilant and use the knowledge we have gained from 1918 and other influenza pandemics to direct targeted research and pandemic influenza preparedness planning, emphasizing prevention, containment, and treatment.” (Morens, Taubenberger, Harvey and Memoli 2010). Of course, planning and prevention are notable features of public health systems, but quite scarce in systems that rely on private health care (Anderson 2007).
Nevertheless, even in the USA which has never had a well-developed public health system, components of a pandemic plan were utilized during the 1918–1919 flu crisis. There was “coordination between different levels and branches of government, improved communications … mass dispensing of vaccines, guidelines for infection control, containment measures including case isolation and closures of public places, and disease surveillance”, which were employed “with varying degrees of success” (Ott, Shaw, Danila and Lynfield 2007). Today the US maintains a Centre for Disease Control and Prevention (CDC), but it lacks a universal health guarantee and carries the burden of corporatized ‘managed care’ (Sekhri 2000).
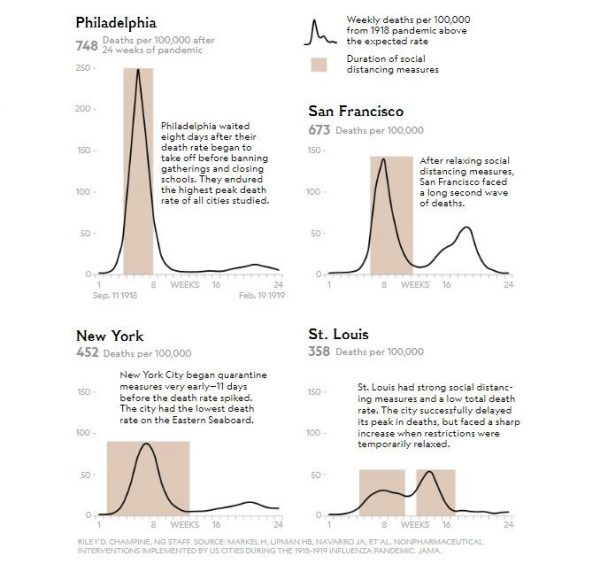
There are some important lessons from the US experience in 1918-1919. Strochlic and Champine (2020) stress the danger of relaxing restrictive quarantine measures too soon – those US cities that kept social closures for some weeks after the peak of casualties avoided a second ‘spike’ and had the lowest overall death rates. Unlike New York today under COVID-19, a city with the highest rates of infection, New York City in 1918 began its quarantine measures early and kept them for four weeks after the spike in deaths. It then had “the lowest death rate of the eastern seaboard”. San Francisco, St Louis and some other cities, which ended their quarantine measures earlier, had a second round of deaths and a second round of quarantine restrictions (Strochlic and Champine 2020). See Graphic 1 below. So the lesson here is to implement quarantine measures (1) early and (2) keep them going for some weeks after the peak in deaths.
In Spain, the epidemic was first widely reported in late May 1918. Rates of death from influenza shot up, but the first epidemic seemed to have ended in 2 months. However, a second epidemic began slowly in September, peaking in October. No antibiotics were then available for pneumonia, which was usually the final killer. A third and final period of the epidemic was from January to June 1919. Deaths were more common amongst babies and young people and more than 260,000 (1% of the Spanish population) died (Trilla, Trilla and Daer 2008).
So the current pandemic restrictive measures are not new: quarantine regimes including distancing and the wearing of masks, while treatments are developed and a vaccine to accelerate social immunity is found. Isolation measures, closures of social facilities and social distancing must be developed according to local circumstances, preferably with popular education and broad social consent. Such measures are particularly important to slow the epidemic, especially when there is limited knowledge of how to treat and contain it.
There is a consensus on this across many different countries. George Gao, head of the Chinese CDC says “social distancing is the essential strategy for the control of any infectious diseases, especially if they are respiratory infections”. “Non-drug measures” are particularly important, especially without clear knowledge of the appropriate drugs. This social distancing generally includes isolating those with the infection, quarantining their close contacts, suspending social gatherings and restricting movement, if not complete lockdowns (Cohen 2020). It has been suggested that, with general quarantine measures “compliance of below 70% is unlikely to succeed for any duration of social distancing, while a compliance at the 90% level is likely to control the disease within 13–14 weeks, when coupled with effective case isolation and international travel restrictions” (Chang, Harding, Zachreson, Cliff and Prokopenko 2020). More targeted quarantine measures would require large scale testing.
The phenomenon of ‘herd immunity’ can occur in two ways, (1) by ‘natural selection’, where largescale death will claim many and only those able to develop auto-immunity survive; or (2) by an accelerated method where a vaccine is given to rapidly increase the numbers of those with antibodies for the particular virus. This both slows down transmission and protects those with transmitted immunity (Regalado 2020). The wide use of mass vaccines across the 20th century saved millions of lives, from diseases such as smallpox, polio, cholera and measles. At least 16 vaccines for COVID-19 are under testing at the time of writing (Akst 2020), and estimates of availability range from two to eighteen months.
3. Differential impact
Even as COVID19 infection rates remain high in much of Europe and the USA, we can see important differences across countries in the impact, management, and recovery from the virus. Interpreting interim data is difficult but necessary, if we are to learn contemporary lessons. The first obstacles to reading the data are that there is under-reporting and low levels of testing. Problems for learning also come from the commitment, in many countries, to highly privatized health systems. These are notoriously weak in preventive health and crisis management, There is also a great resistance in western societies to learning from other cultures. For example, it has been pointed out that when China was in the midst of its crisis, with hundreds dying, this was cited in western circles as “proof their government was incompetent”; yet when China’s infection rates fell this was said to be “proof they were lying about numbers” (Mastracci 2020). Not so many were ready to learn from China.
We have to recognize some caveats about the use of contemporary, interim data. Although the WorldOmeter site collates COVID19 data from governments and seems to do this fairly reliably, the state reports do vary considerably. Yet it is easy to check, for example, the published government data from (e.g.) the UK, South Korea and the USA (GOV.UK 2020, KCDC 2020 and CDC 2020) against that collated at WorldOmeter. Nevertheless, this raw data has to be treated with caution. Some useful caveats on using this epidemic data were spelled out in an article on the BBC. Henriques (2020) pointed out that the varied scale of testing will have a great impact on cited infections, suggesting that the “lack of widespread, systematic in most countries is probably the main source of discrepancies in death rates internationally” (Henriques 2020). As it happens, information on the level of testing in many countries has since become available. Henriques also points out the difference between ‘dying with’ and ‘dying from’ the disease, including the fact that the reasons for medical registration of death vary between countries. The H1N1 epidemic of 2009 also showed wide cross-country variation in death rates, and some of the higher rates were later revised downwards when better information was available (Vaillant, La Ruche, Tarantola and Barboza 2009). Conversely, deaths may also be underestimated, as many are never tested. Most likely, infection rates are more unreliable than the death rates, due to under-reporting and lack of testing. Finally, levels of bacterial resistance (important in the case of pneumonia, a major cause of COVID19 related death) may vary between countries. Differing demographics are also important. For example, there are said to be proportionally twice as many Italians over 65 years of age as there are Chinese (Henriques 2020). These are important factors to bear in mind, but should not deter us from making use of the best available evidence. Commentary without evidence is guesswork.
It is important to discuss, in particular, why the UK and US reactions and disease control seem to have been so poor. The Anglo-American duo has been presented, by UK and US agencies, as at the peak of “international preparedness for epidemics and pandemics” in measures of ‘Global Health Security’ (IPT 2020). Yet virtually none of the impact data supports that claim. Daily deaths from COVID19 in China began to fall in late February, to just a handful each day in the first week of April. In that same first week of April, the USA was suffering more than one thousand deaths every day and the UK around 500 or more deaths every day (WorldOmeter 2020). Why did these two wealthy countries fare so badly?
The UK and USA reacted very slowly to the pandemic and, by early April when cases and deaths had fallen in China and South Korea, and were peaking in much of Europe (by late March in Italy and Spain), US and UK rates were still rising (Burn-Murdoch 2020). On 10 April COVID19 linked deaths were 4 times (in the USA) and 9 times (in the UK) the global average (WorldOmeter 2020). By that time the rate of testing in both countries was comparable and relatively high. Table 1 below shows testing in the UK rising strongly only in early April. This table has no data for China, but we have other sources which show that Chinese testing was intense, at least in the affected provinces.

Guangdong province “did more than 320 000 RT-PCR tests on those who had attended fever clinics and hospitals over 30 days between January and February 2020”. This was “about ten times the baseline testing capacity for routine influenza-like illness surveillance during the influenza season of 2018” (Forster, Forster, Renfrew and Forster 2020). Indeed, the Chinese were the first to sequence and publish the genome of the virus, in mid-January, and to develop tests (Cohen 2020a). At the time of writing, “of 202 companies around the world producing commercialized Covid-19 test kits, 92 are from China” (Cookson and Hodgson 2020). WHO official Bruce Aylward pointed out that China had to innovate to stop the first largescale outbreak of the virus, and to isolate and quarantine those found to be infected. That meant testing. Yet as late as mid-March the UK government announced that it would only test for COVID-19 among people admitted to hospital and that people with mild symptoms wouldn’t be tested but should simply stay at home for seven days” (Hamzelou 2020).
By way of contrast, according to the WHO, South Korea was “pretty rigorous about testing all the suspect cases and finding all the contacts … [and so] they seem to have turned a corner” (Hamzelou 2020). The much lower death rate in South Korea tends to bear that out. The contrast with an indecisive UK approach was noted.
“In contrast with the early stages in the UK – where Boris Johnson said coronavirus was likely to “spread a bit more”, South Korean health officials quickly learned the lessons from Wuhan … [they] prioritized identifying and isolating people testing positive for the disease, and developed capacity to run about 15,000 diagnostic tests a day” (Beaumont 2020).
Other sources noted the early high levels of testing in China and South Korea, including many who had no symptoms of illness. “Widespread testing” in China, Iceland and South Korea “identified a high proportion of infections in people without discernible symptoms” (Gale 2020). The Chinese Centre for Disease Control and Prevention developed the earliest tests and “details of it were posted on the World Health Organization website on 24 January, just after the Wuhan lockdown was announced”. By late March China had conducted “well over 320,000 tests” (Beaumont 2020). Cookson and Hodgson (2020) wrote that “Germany and South Korea have led the way in rolling out tests on a large scale, but the UK and US have been laggards”.
It has emerged that US military bases and some warships have become strong sources of infection and likely also international transmission (Arkin 2020), as indeed they were a century ago, with the so-called ‘Spanish flu’. That remains an as-yet unaddressed threat to the US population and the international community, given that the US has nearly 800 military bases around the world (Vine 2015). Crowded prisons have become an additional hotbed of COVID19 infection, and the US has the biggest prison system and the highest imprisonment rate on earth (Wagner and Sawyer 2018). This threatens the lives of prisoners and staff (Yan 2020) and creates a hotline of community transmission because, contrary to popular belief, there is constant high-level traffic between prisons and wider communities. There is little sign that either the US military or prison authorities have a plan to deal with these threats.
In the absence of a vaccine, drug treatments varied considerably, although similar drugs were potentially available. One large survey of more than 6,000 physicians from 30 countries sheds some light on the disparity. Substantial differences can be seen between the US and Chinese doctors. The survey question was “of the medications you have personally prescribed or have seen used, please indicate which ones are most effective”. The results are shown in Table 2 below.
The most striking differences are that very many US doctors often regarded no medication as the best option, while Chinese doctors made far greater use of anti-viral or immunotherapy drugs, and a type of pre-vaccine treatment of plasma from recovered patients. In early February the Cuban interferon variant (Interferon Alpha-2B Recombinant: IFNrec) was also being used in China, in combination with the anti-virals (Telesur 2020; O’Connor 2020). The top “more information topic” all doctors requested was more on “the efficacy of existing medicines” (Sermo 2020: 19). Clearly there was uncertainty, but Chinese doctors were using more sophisticated medication. Why were US doctors more reluctant to use anti-virals? First, they could not use the Cuban version of interferon because of the economic blockade imposed by their government against Cuban products (O’Connor 2020). Second, it seems likely that the medical consensus in the USA – dominated as it is by large private health corporations, managed care and expensive patented medicines – would not easily countenance the provisional use of unproven and expensive antivirals. In China, on the other hand, the antivirals were likely much more affordable.
Western scientists have acknowledged that the speed in vaccine development “is thanks in large part to early Chinese efforts to sequence the genetic material of Sars-CoV-2, the virus that causes Covid-19. China shared that sequence in mid-January (Spinney 2020; Cohen 2020a). By early April, vaccines in development were said to include two “frontrunners” in the US, one in China and one in the UK, all of which had clinical trials underway. Another 11 were in development (Akst 2020). In addition, the Hong Kong listed CanSino Biologics has a vaccine project with the Chinese military (Bloomberg 2020) and the UK giant GlaxoSmithKline has a collaborative vaccine project with China’s Xiamen Innovax Biotech (Taylor 2020). There is clearly a race to produce first and to be recognized as safe and effective. Billions of dollars are at stake, as well as many thousands of lives. No doubt there will be a war of words when the first vaccines emerge. Estimates of vaccine readiness vary from two months to 18 months. However, it seems likely that the Chinese companies, in particular, will fast track their process.
With the uncertainty about treatment and in the absence of a vaccine, ‘non-pharmaceutical’ means of containing the spread of the virus became important. That meant quarantine measures and limits on movement and association, to prevent an escalation of contagion. These measures must necessarily be tailored to particular circumstances and, to justify any curtailment of civil liberties, should be ‘proportionate’ to the particular threat posed. The UN Human Rights Committee’s General Comment on Article 12 (‘Freedom of Movement’) of the International Covenant on Civil and Political Rights, explains proportionality in this way:
“Restrictive measures must conform to the principle of proportionality; they must be appropriate to achieve their protective function; they must be the least intrusive instrument amongst those which might achieve the desired result; and they must be proportionate to the interest to be protected.” (HRC 1999: 14)
In this sense, restrictive measures during the pandemic must relate to the threat and should be relaxed when the threat has diminished. Since a wide variety of restrictive measures have been imposed across a large range of countries, it necessarily falls to citizens of those places to demand accountability, full explanations and the best targeted and “least intrusive” measures. Nevertheless, as mentioned above, during the 1918 epidemic in the USA, the cities that relaxed too soon were hit by a second wave (Strochlic and Champine 2020). That potential threat is a relevant consideration. So the public health and civil rights logic are for gradual relaxation which allows for control of transmission, until proper treatment is found. A Chinese study on preventing a second wave of infections was widely misreported as saying that “lockdowns shouldn’t be fully lifted until coronavirus vaccine found” (Reynolds 2020). In fact that study calls for a gradual response, with vigilance to “allow policymakers to tune relaxation decisions to maintain [low] transmissibility” (Leung, Wu, Liu and Leung 2020).
On quarantine, once again, we see big differences between China and the USA. In Wuhan, once the new virus was detected, there was an early and severe lockdown of the city and to some extent Hubei province, to prevent it from spreading to the rest of the country. That was only relaxed after 76 days, several weeks after new infections had peaked and fallen (CGTN 2020). In the US the restrictions were at first aimed at the supposed source in China, then others were imposed quite late. The US national health system, such as it is, was poorly equipped to manage the process. Washington moved slowly and indecisively, with a series of complacent and repeated assurances throughout February from President Trump, that “we have it very well under control” (Brewster 2020; Guerra 2020). Similarly, British leader Boris Johnson was accused of complacency, being “slow to act” and even suggesting that some natural “herd immunity” might be necessary. This sounded like the UK government “was deliberately aiming for 60 percent of the populace to fall ill” (Stewart, Weaver and Proctor 2020; Yong 2020). Without vaccine assisted “herd immunity”, such an approach would mean tens and perhaps hundreds of thousands could die. As it turned out, Johnson himself contracted the virus and was hospitalized.
The rapid and strict Chinese measures seemed to contain the spread of the virus in Wuhan and some contiguous central provinces, while other provinces were less unaffected (Fan et al 2020). Another study showed a similar pattern, with western, northern and some of the eastern provinces relatively unaffected (Guan et al 2020). China’s prompt and comprehensive measures (early detection, massive localized testing including temperature monitoring, treating, contact tracing and quarantine) allowed the hardest hit area, Wuhan, to gradually emerge from severe quarantine restrictions after 76 days. That city now has a color-coded, graduated system to allow progressively greater freedom to move around (Galindo 2020). In the USA the ‘hot spots’ have been New York and New Jersey, but very quickly high levels of infection, including community transmission, were reported on the west coast (California, Washington), in the great lakes area (Illinois, Michigan) and in the southeast (Louisiana, Florida) (CDC 2020). By 9 April twelve US states had death rates of 35 per million, more three times the reported global average (WorldOmeter 2020).
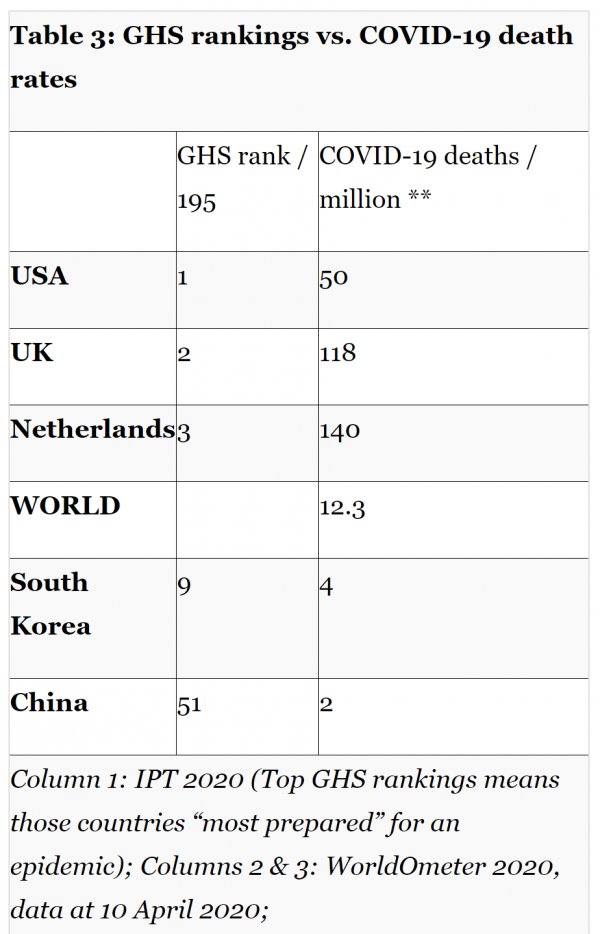
Amongst the many institutional failures has been the failure to predict better ‘preparedness’ for such an epidemic. The crisis poses a great challenge to US ideology, based as it has been on corporate privilege and a belief in US technological superiority. In the past this neo-colonial approach was linked to the rationale of ‘market solutions’. For example, in late 2019 an Anglo-American group created a ‘Global Health Security Index’ which ranked the USA at the top of countries able to deal with “infectious disease outbreaks that can lead to international epidemics and pandemics”; the UK was number two (IPT 2020). Yet after three months of the COVID-19 pandemic many of the GHS rankings seem absurd, with the top three (USA, UK and The Netherlands) showing significantly worse than world average fatality rates from COVID-19. Of the highly ranked GHS countries, only South Korea showed some consistency between GHS ranking and superior performance. See Table 3 below.
Since all the above states, by early April, had fairly high and comparable levels of testing (4,400 to 9,300 per million), and as death rates are more reliable than infection rates, we are entitled to use death rates as a rough inverse measure of epidemic preparedness. That is, unless we assume that the full extent of the virus has not yet been measured, or that the virus may be about to recur in China or Korea. There is not much reason, at this stage, to imagine that under-reporting of death is better or worse in any of those states.
Indeed South Korea, with an early and strong testing regime (KCDC 2020), was able to carry out more selective quarantine measures, “to make tactical decisions regarding schools … movements … to move forward without some of the draconian measures”, and this allowed it to keep many factories, shopping malls and restaurants open (Beaubien 2020).
This brings us to the ‘anti-authoritarian’ argument, used by the Anglo-American duo. Both the US and the UK have either rejected a full, well-coordinated public health system (the US) or undermined it (in the UK) on the grounds of ‘liberty’ and the ‘authoritarian’ nature of large, well-resourced public health systems. Yet both, once they realized the scale of the epidemic, resorted to their police and armed forces to control civilian populations, recognizing that such measures were beyond the capacity of their health workforce (Haynes 2020; Browne 2020). Where restrictive measures are imposed early by local health authorities, there is more likely to be understanding and compliance.
4. Lessons
There is also the question of culture and broader social cohesion. It has been suggested that eastern countries like South Korea and China have done better because of the “deep divisions and poor leadership in the west”, and that “the trust that citizens must have in governments is low in the west and that has hurt its ability to mobilize people in a time of grave peril” (Chaulia 2020). The cynical reactions to the erratic behavior of the UK and US leaders lend some support to this claim. The western stereotype is often that “authoritarian” systems fail from suppressing information and communications (Gebrekidan 2020). But the suggested authoritarian-liberal dichotomy is a false one, because the late entry of the US and UK to quarantine restrictions was accompanied by severe policing, severe penalties, the use of police drone surveillance and the domestic deployment of armed forces (Castle 2020; Haynes 2020; Browne 2020). All public health systems are paternalistic, or maternalistic, but the use of armed forces due to incapacity in the public health system is a serious failing.
There are important lessons from China, as from principles drawn from past epidemic management, and the crisis has exposed weaknesses in the US and UK systems. The social mobilization in Wuhan, organized by local authorities and backed by the central government, certainly helped early recovery from what could have been an even more devastating epidemic (Leung, Wu, Liu and Leung 2020). Other countries cannot copy that experience, but they can observe and draw lessons (CGTN 2020).
Early restrictive and quarantine measures were in principle justified, but by international law they should be ‘proportionate’ to the particular threat posed and employing the ‘least restrictive’ measures possible. Public health logic accepts that restrictions on movement and association should be relaxed as the infection rates abate, in coordination with an epidemiological vigilance to ensure that a second wave of infections does not arise (Leung, Wu, Liu and Leung 2020; EurekAlert 2020). Time frames should reassure populations that there is some end in sight to restrictive measures, and that relaxation can begin even before vaccines are available, when the disease is controlled.
It seems likely that greater experimentation with the use of anti-viral and immunotherapy drugs helped treatment in China, but this was impeded in the USA, where strong patent laws and corporate management make the newer forms of such drugs expensive. There is now strong competition to produce the first vaccine, and for that reason level some availability seems likely within two months. However, we can expect to see a war of words between the companies involved, over questions of safety and efficacy.
Overall, countries such as the US and the UK, which had weak or run down public health systems, failed their own peoples by predictable deficits in preparedness, health workforces, protective equipment, preventive capacity, early detection and swift responses. When they did respond they tended to draw on security forces in lieu of an effective health workforce. Death rates were far higher than average and recovery may take longer. In the case of the US, the deficit is compounded by serious infection in the 150 military bases at home and the 800 US military bases abroad. Those pose a risk to the US population and to the many host countries. China and South Korea did better through their universal health cover, greater investment in health systems and greater commitment to health crisis planning.
References
Akst, Jef (2020) ‘COVID-19 Vaccine Frontrunners’, The Scientist, 7 April, online: https://www.the-scientist.com/news-opinion/covid-19-vaccine-frontrunners-67382
Andersen, Kristian G., Andrew Rambaut, W. Ian Lipkin, Edward C. Holmes & Robert F. Garry (2020) The proximal origin of SARS-CoV-2, 17 March, online: https://www.nature.com/articles/s41591-020-0820-9
Anderson, Tim (2007) ‘Health, income and public institutions: explaining Cuba and Costa Rica’, New School Economic Review, Volume 2(1), 22-37
AP (2020) ‘Cuban Docs Fighting Coronavirus Around World, Defying US’, New York Times, 3 April, online: https://www.nytimes.com/aponline/2020/04/03/world/europe/ap-cb-virus-outbreak-cuban-doctors.html
Arkin, William (2020) ‘First Public map reveals military bases with coronavirus cases as Pentagon secrecy draws backlash’, 9 April, Newsweek, online: https://www.newsweek.com/exclusive-first-public-map-reveals-military-bases-coronavirus-cases-pentagon-secrecy-draws-1496951
Barry, John M. (2004) ‘The site of origin of the 1918 influenza pandemic and its public health implications’, J Transl Med. 2004; 2: 3. 20 Jan. doi: 10.1186/1479-5876-2-3, online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC340389/
BBC (2020) ‘China coronavirus: Misinformation spreads online about origin and scale’, 30 January, online: https://www.bbc.com/news/blogs-trending-51271037
Beaubien, Jason (2020) ‘How South Korea Reined In The Outbreak Without Shutting Everything Down, NPR, 26 March, online: https://www.npr.org/sections/goatsandsoda/2020/03/26/821688981/how-south-korea-reigned-in-the-outbreak-without-shutting-everything-down
Beaumont, Peter (2020) ‘Coronavirus testing: how some countries got ahead of the rest’, The Guardian, 2 April, online: https://www.theguardian.com/world/2020/apr/02/coronavirus-testing-how-some-countries-germany-south-korea-got-ahead-of-the-rest
Bergna, Annalisa (2020) ‘Coronavirus Diaries: I’m a Biologist in Milan Working Nonstop to Understand COVID-19’, Slate, 18 March, online: https://slate.com/technology/2020/03/coronavirus-milan-biologist-sequencing.html
Bloomberg (2020) ‘Chinese Vaccine Approved for Human Testing at Virus Epicenter’, 18 March, online: https://www.bloomberg.com/news/articles/2020-03-18/chinese-vaccine-approved-for-human-testing-at-virus-epicenter
Brewster, Jack (2020) ‘Fauci Says It’s ‘False’ To Say The Coronavirus Outbreak Is Under Control; Here Are All The Times Trump Said It Was’, Forbes, 5 April, online: https://www.forbes.com/sites/jackbrewster/2020/04/05/fauci-says-its-false-to-say-the-coronavirus-outbreak-is-under-control-here-are-all-the-times-trump-said-it-was/
Browne, Ryan (2020) ‘US military preparing to deploy additional forces to support coronavirus response’, 3 April, CNN, online: https://edition.cnn.com/2020/04/03/politics/us-military-additional-forces-coronavirus/index.html
Burnet, F.M. and Ellen Clark (1942) Influenza: a survey of the last fifty years, MacMillan, Melbourne
Burn-Murdoch, John (2020) ‘Coronavirus outbreaks plateau in Italy and Spain’, Financial Times, 3 April, online: https://www.ft.com/content/c764b98d-ae03-41ac-a2ca-8309f32d5e1c
Castle, Stephen (2020) ‘To Enforce Coronavirus Rules, U.K. Police Use Drones, Shaming and Easter Egg Bans’, New York Times, 1 April, online: https://www.nytimes.com/2020/04/01/world/europe/uk-police-coronavirus.html
CDC (2020) ‘Coronavirus Disease 2019 (COVID-19): cases in US, online: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
CGTN (2020) ‘What does Wuhan tell us?’, 8 April, online: https://www.youtube.com/watch?v=q_z7dX4lGl0
Chang, Sheryl L.; Nathan Harding, Cameron Zachreson, Oliver M. Cliff and Mikhail Prokopenko (2020) ‘Modelling transmission and control of the COVID-19 pandemic in Australia’, 3 April, online: https://arxiv.org/pdf/2003.10218.pdf
Chaulia, Sreeram (2020) ‘Why East beats West in the war against coronavirus’, RT, 27 March, online: https://www.rt.com/op-ed/484298-east-west-war-coronavirus/
Cohen, Jon (2020a) ‘Chinese researchers reveal draft genome of virus implicated in Wuhan pneumonia outbreak’, Science Mag, 11 january, online: https://www.sciencemag.org/news/2020/01/chinese-researchers-reveal-draft-genome-virus-implicated-wuhan-pneumonia-outbreak
Cohen, Jon (2020) ‘Not wearing masks to protect against coronavirus is a ‘big mistake,’ top Chinese scientist says’, Science Mag, 27 March, online: https://www.sciencemag.org/news/2020/03/not-wearing-masks-protect-against-coronavirus-big-mistake-top-chinese-scientist-says
Cookson, Clive and Camilla Hodgson (2020) ‘What coronavirus tests does the world need to track the pandemic?, Financial Times, 1 April, online: https://www.ft.com/content/0faf8e7a-d966-44a5-b4ee-8213841da688
Dai, Candace Tran (2009) ‘New Reforms to the Health System’, China perspectives, , No. 3 (79), pp. 108-109
Doherty, Peter (2020) ‘The pandemic we had to have’, The Saturday Paper, 28 March, online: https://www.thesaturdaypaper.com.au/opinion/topic/2020/03/28/the-pandemic-we-had-have/15853140009591
EurekAlert (2020) ‘The Lancet: Modelling study estimates impact of relaxing control measures on possible second wave of COVID-19 in China’, 8 April, online: https://www.eurekalert.org/pub_releases/2020-04/tl-pss040820.php
Fan, Jingchun; Xiaodong Liu, Weimin Pan, Mark W. Douglas, and Shisan Bao (2020) ‘Epidemiology of 2019 Novel Coronavirus Disease-19 in Gansu Province, China, 2020’, Emerging Infectious Diseases, Volume 26, Number 6—June 2020, online: https://wwwnc.cdc.gov/eid/article/26/6/20-0251_article
Forster, Peter; Lucy Forster, Colin Renfrew, and Michael Forster (2020) ‘Phylogenetic network analysis of SARS-CoV-2 genomes’, PNAS, 8 April, online: https://www.pnas.org/content/early/2020/04/07/2004999117
Gale, Jason (2020) ‘Coronavirus Testing in China Finds More Symptom-Free Cases’, Bloomberg, 3 April, online: https://www.bloombergquint.com/global-economics/fresh-coronavirus-testing-in-china-finds-more-symptomless-cases
Galindo, Ana (2020) ‘Wuhan will emerge from the closure after 76 days’, Viral Newsity, March 27, online: https://viralnewsity.com/wuhan-will-emerge-from-the-closure-after-76-days/
Gallón, Natalie (2020) ‘Bodies are being left in the streets in an overwhelmed Ecuadorian city’, CNN, 4 April, online: https://edition.cnn.com/2020/04/03/americas/guayaquil-ecuador-overwhelmed-coronavirus-intl/index.html
Gebrekidan, Selam (2020) ‘For Autocrats, and Others, Coronavirus Is a Chance to Grab Even More Power’, New York Times, 30 March, online: https://www.nytimes.com/2020/03/30/world/europe/coronavirus-governments-power.html
GOV.UK (2020) ‘Number of coronavirus (COVID-19) cases and risk in the UK’, online: https://www.gov.uk/guidance/coronavirus-covid-19-information-for-the-public
Guan, Wei-jie et al (2020) ‘Clinical Characteristics of Coronavirus Disease 2019 in China’, New England Journal of Medicine, 28 February, online: https://www.nejm.org/doi/full/10.1056/NEJMoa2002032
Guerra, Angel (2020) ‘Trump y la negación del coronavirus’, La Jornada, 26 March, online: https://www.jornada.com.mx/2020/03/26/opinion/024a1mun
Hamzelou, Jessica (2020) ‘WHO expert: We need more testing to beat coronavirus’, New Scientist, 16 March, online: https://www.newscientist.com/article/2237544-who-expert-we-need-more-testing-to-beat-coronavirus/
Haynes, (2020) ‘Coronavirus: Armed forces rapidly expand their response to COVID-19’, Sky News, 7 April, online: https://news.sky.com/story/coronavirus-armed-forces-rapidly-expand-their-response-to-covid-19-11970136
Henriques, Martha (2020) ‘Coronavirus: Why death and mortality rates differ’, BBC, 2 April, online: https://www.bbc.com/future/article/20200401-coronavirus-why-death-and-mortality-rates-differ
Holland, Kate (2020) ‘Sorry, conspiracy theorists. Study concludes COVID-19 ‘is not a laboratory construct’, ABC News, 27 March, online: https://abcnews.go.com/US/conspiracy-theorists-study-concludes-covid-19-laboratory-construct/story
HRC (1999) ‘Human Rights Committee, General Comment 27, Freedom of Movement (Art.12), U.N. Doc CCPR/C/21/Rev.1/Add.9, online: http://hrlibrary.umn.edu/gencomm/hrcom27.htm
Huang, Chaolin et al (2020) ‘Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China’, The Lancet, 15 February, online: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30183-5/fulltext
IPT (2020) ‘Global Health Security Index’, Index Project Team (IPT) [comprising the Nuclear Threat Initiative (NTI), the Johns Hopkins Center for Health Security (JHU) and The Economist Intelligence Unit (EIU)], online: https://www.ghsindex.org
KCDC (2020) ‘The updates on COVID-19 in Korea’, online: https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030
Kwon S, Lee Tj, Kim Cy (2015) ‘Republic of Korea Health System Review’, Vol.5 No.4. World Health Organization, Manila
Leung, Kathy; Joseph T. Wu, Di Liu and Gabriel M. Leung (2020) ‘First-wave COVID-19 transmissibility and severity in China outside Hubei after control measures, and second-wave scenario planning: a modelling impact assessment’, The Lancet, 8 April, online: https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(20)30746-7.pdf
Mastracci, Davide (2020) ‘Don’t Blame China For Your Government’s COVID-19 Failures’, Passage, 7 April, online: https://readpassage.com/dont-blame-china-for-your-governments-failure-to-contain-covid-19/
Morens, David M; Jeffery K. Taubenberger, Hillery A. Harvey, and Matthew J. Memoli,
(2010) ‘The 1918 influenza pandemic: Lessons for 2009 and the future’, Crit Care Med. 2010 Apr; 38(4 Suppl): e10–e20, online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3180813/
New China TV (2020) ‘CDC director says some COVID-19 deaths diagnosed as flu-related in U.S.’, 12 March, online: https://www.youtube.com/watch?v=Y_dU2RCqWs4
O’Connor, Tom (2020) ‘Cuba uses ‘wonder drug’ to fight Coronavirus around the world despite U.S. sanctions’, Newsweek, 24 March, online.
Ott, Miles; Shelly F. Shaw, Richard N. Danila, and Ruth Lynfield (2007) ‘Lessons Learned from the 1918–1919 Influenza Pandemic in Minneapolis and St. Paul, Minnesota’, Public Health Reports, Nov-Dec; 122(6): 803–810, online.
Poggioli, Sylvia (2020) ‘’Every Single Individual Must Stay Home’: Italy’s Coronavirus Surge Strains Hospitals’, NPR, 19 March, online.
Qingyue M, Hongwei Y, Wen C, Qiang S, Xiaoyun L. (2015) ‘People’s Republic of China Health System Review’, Vol.5 No.7. World Health Organization, Manila
Regalado, Antonio (2020) ‘What is herd immunity and can it stop the coronavirus?’, MIT Technology Review, 17 March, online.
Reynolds, Emma (2020) ‘Lockdowns shouldn’t be fully lifted until coronavirus vaccine found, new study warns’, CNN, 9 April, online.
Sekhri, Neelam K. (2000) ‘Managed care: the US experience’, Bulletin of the World Health Organization, 78 (6), 830-844, online.
Stewart, Heather; Mathew Weaver and Kate Proctor (2020) ‘’Nonchalant’: Boris Johnson accused of Covid-19 complacency’, The Guardian, 28 March, online.
Strochlic, Nina and Riley D. Champine (2020) ‘How some cities ‘flattened the curve’ during the 1918 flu pandemic’, National Geographic, 27 March, online.
Sermo (2020) ‘Sermo’s COVID-19 Real Time Barometer Study’, 25-27 March, online.
Spinney, Laura (2020) ‘When will a coronavirus vaccine be ready?’, The Guardian, 7 April, online.
Sullivan, Peter (2020) ‘Ohio health official estimates 100,000 people in state have coronavirus’. The Hill, 12 March, online.
Taylor, Nick Paul (2020) ‘GSK allies with Innovax for COVID-19 vaccine R&D project’, Fierce Biotech, 3 April, online.
Telesur (2020) ‘Chinese Doctors Are Using Cuban Antivirals Against Coronavirus’, 6 February, online.
Trilla, Antoni; Guillem Trilla, Carolyn Daer (2008) ‘The 1918 “Spanish Flu” in Spain’, Clinical Infectious Diseases, Volume 47, Issue 5, 1 September 2008, Pages 668–673, https://doi.org/10.1086/590567
Vaillant, L; G La Ruche1, A Tarantola, P Barboza (2009) ‘Epidemiology of fatal cases associated with pandemic H1N1 influenza 2009’, Eurosurveillance, Volume 14, Issue 33, 20/Aug/2009, online.
Vine, David (2015) ‘Where in the World Is the U.S. Military?’, July-August, Politico, online.
Wagner, Peter and Wendy Sawyer (2018) ‘States of Incarceration: The Global Context 2018’, Prison Policy Initiative, June, online.
WHO (2018) ‘Managing epidemics’, World Health Organization, online.
WorldOMeter (2020) COVID-19 CORONAVIRUS PANDEMIC, online.
Wyatt, Tim (2019) ‘Research into deadly viruses and biological weapons at US army lab shut down over fears they could escape’, The Independent, 6 August, online.
Yan, Holly (2020) ‘Prisons and jails across the US are turning into ‘petri dishes’ for coronavirus. Deputies are falling ill, too’, CNN, 9 April, online.
Yong, Ed (2020) ‘The U.K.’s Coronavirus ‘Herd Immunity’ Debacle’, The Atlantic, 16 March, online.
Yu, Wen Bin; Guang da Tang and R.T. Corlett (2020) ‘Decoding the evolution and transmissions of the novel pneumonia coronavirus (SARS-CoV-2) using whole genomic data’, Research Gate, pre-print, February, online.
Zhao, Lijian (2020) ‘When did patient zero begin in US?’ Twitter, 13 March, online.
Zimmer, Carl (2020) ‘Most New York Coronavirus Cases Came From Europe, Genomes Show’, New York Times, 8 April, online.
Dr. Tim Anderson is Director of the Sydney-based Centre for Counter Hegemonic Studies. He has worked at Australian universities for more than 30 years, teaching, researching and publishing on development, human rights and self-determination in the Asia-Pacific, Latin America and the Middle East. In 2014 he was awarded Cuba’s medal of friendship. He is Australia and Pacific representative for the Latin America based Network in Defence of Humanity. His most recent books are: Land and Livelihoods in Papua New Guinea (2015), The Dirty War on Syria (2016), now published in ten languages; Countering War Propaganda of the Dirty War on Syria (2017) and Axis of Resistance: towards an independent Middle East (2019).
